Glaucoma
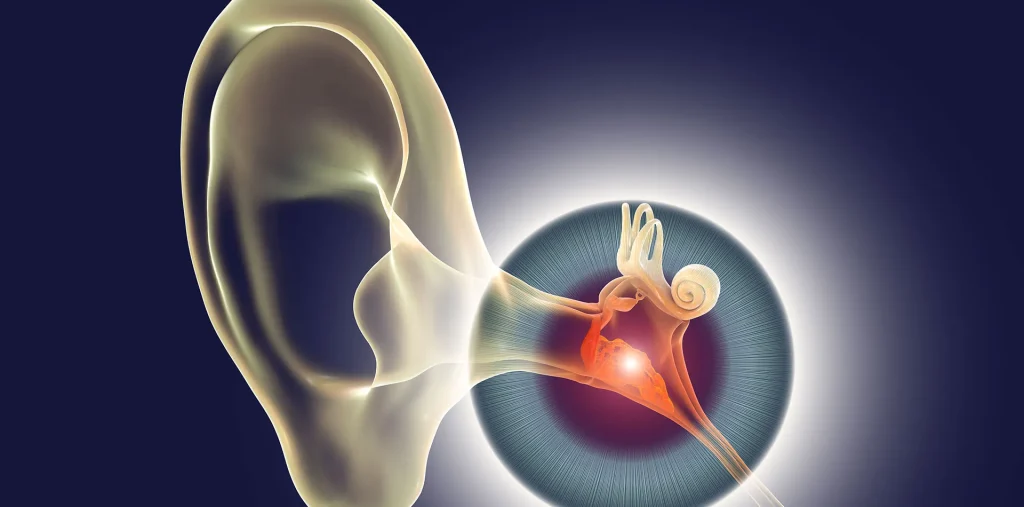
Glaucoma Glaucoma is a group of eye conditions that damage the optic nerve, the health of which is vital for good vision. This damage is often caused by an abnormally high pressure in your eye. Glaucoma is one of the leading causes of blindness for people over the age of 60. It can occur at any age but is more common in older adults. Many forms of glaucoma have no warning signs. The effect is so gradual that you may not notice a change in vision until the condition is at an advanced stage. Because vision loss due to glaucoma can’t be recovered, it’s important to have regular eye exams that include measurements of your eye pressure so a diagnosis can be made in its early stages and treated appropriately. If glaucoma is recognized early, vision loss can be slowed or prevented. If you have the condition, you’ll generally need treatment for the rest of your life. Causes of Glaucoma Glaucoma is the result of damage to the optic nerve. As this nerve gradually deteriorates, blind spots develop in your visual field. For reasons that doctors don’t fully understand, this nerve damage is usually related to increased pressure in the eye. Elevated eye pressure is due to a buildup of a fluid (aqueous humor) that flows throughout the inside of your eye. This internal fluid normally drains out through a tissue called the trabecular meshwork at the angle where the iris and cornea meet. When fluid is overproduced or the drainage system doesn’t work properly, the fluid can’t flow out at its normal rate and eye pressure increases. Glaucoma tends to run in families. In some people, scientists have identified genes related to high eye pressure and optic nerve damage. Types of glaucoma include: Open-angle glaucoma Open-angle glaucoma is the most common form of the disease. The drainage angle formed by the cornea and iris remains open, but the trabecular meshwork is partially blocked. This causes pressure in the eye to gradually increase. This pressure damages the optic nerve. It happens so slowly that you may lose vision before you’re even aware of a problem. Angle-closure glaucoma Angle-closure glaucoma, also called closed-angle glaucoma, occurs when the iris bulges forward to narrow or block the drainage angle formed by the cornea and iris. As a result, fluid can’t circulate through the eye and pressure increases. Some people have narrow drainage angles, putting them at increased risk of angle-closure glaucoma. Angle-closure glaucoma may occur suddenly (acute angle-closure glaucoma) or gradually (chronic angleclosure glaucoma). Acute angle-closure glaucoma is a medical emergency. Normal-tension glaucoma In normal-tension glaucoma, your optic nerve becomes damaged even though your eye pressure is within the normal range. No one knows the exact reason for this. You may have a sensitive optic nerve, or you may have less blood being supplied to your optic nerve. This limited blood flow could be caused by atherosclerosis the buildup of fatty deposits (plaque) in the arteries or other conditions that impair circulation. Glaucoma in children It’s possible for infants and children to have glaucoma. It may be present from birth or develop in the first few years of life. The optic nerve damage may be caused by drainage blockages or an underlying medical condition. Pigmentary glaucoma In pigmentary glaucoma, pigment granules from your iris build up in the drainage channels, slowing or blocking fluid exiting your eye. Activities such as jogging sometimes stir up the pigment granules, depositing them on the trabecular meshwork and causing intermittent pressure elevations. Symptoms of Glaucoma The signs and symptoms of glaucoma vary depending on the type and stage of your condition. For example: Open-angle glaucoma Acute angle-closure glaucoma N.B – If left untreated, glaucoma will eventually cause blindness. Even with treatment, about 15 percent of people with glaucoma become blind in at least one eye within 20 years. When to see a doctor Promptly go to an emergency room or an eye doctor’s (ophthalmologist’s) office if you experience some of the symptoms of acute angle-closure glaucoma, such as severe headache, eye pain and blurred vision. Risk factors Because chronic forms of glaucoma can destroy vision before any signs or symptoms are apparent, be aware of these risk factors: Prevention These self-care steps can help you detect glaucoma in its early stages, which is important in preventing vision loss or slowing its progress. Get regular dilated eye examinations. Regular comprehensive eye exams can help detect glaucoma in its early stages, before significant damage occurs. As a general rule, the American Academy of Ophthalmology recommends having a comprehensive eye exam every five to 10 years if you’re under 40 years old, every two to four years if you’re 40 to 54 years old; every one to three years if you’re 55 to 64 years old, and every one to two years if you’re older than 65. If you’re at risk of glaucoma, you’ll need more frequent screening. Ask your doctor to recommend the right screening schedule for you. Know your family’s eye health history. Glaucoma tends to run in families. If you’re at increased risk, you may need more frequent screening. Exercise safely. Regular, moderate exercise may help prevent glaucoma by reducing eye pressure. Talk with your doctor about an appropriate exercise program. Take prescribed eyedrops regularly. Glaucoma eyedrops can significantly reduce the risk that high eye pressure will progress to glaucoma. To be effective, eyedrops prescribed by your doctor need to be used regularly even if you have no symptoms. Wear eye protection. Serious eye injuries can lead to glaucoma. Wear eye protection when using power tools or playing highspeed racket sports in enclosed courts. Diagnosis Your doctor will review your medical history and conduct a comprehensive eye examination. He or she may perform several tests, including: Treatment The damage caused by glaucoma can’t be reversed. But treatment and regular checkups can help slow or prevent vision loss, especially if you catch the disease in its early stages. Glaucoma is treated by lowering your eye pressure (intraocular